
She does not call it addiction. She calls it "falling too hard." She says she cannot seem to stop going back to him, even though she knows the relationship is damaging. She spends hours thinking about the numerous past relationships, texting and deleting, scrolling dating apps, planning, fantasizing, not because she wants to, exactly, but because the pull is stronger than her intention to stop.
She came to me describing anxiety and low self-esteem. It took several sessions before the fuller picture emerged: a pattern of compulsive sexual and romantic behavior spanning years, followed each time by the same wave of shame and the same vow to change. A pattern she had never named, because there is no name in her world for a woman who experiences this.
The clinical picture for men and women looks different, but the silence looks the same. Men who struggle with compulsive sexual behavior are more likely to recognize it and more likely to seek help. Women are more likely to absorb the shame, reframe the pattern as a relationship problem, and wait.
The Numbers Behind the Silence
The largest cross-cultural study on compulsive sexual behavior to date, the International Sex Survey (Bőthe et al., 2023), collected data from 82,243 participants across 42 countries and found that 2.42% of women and 8.17% of men scored at high risk for Compulsive Sexual Behavior Disorder (CSBD). Across Western population samples, estimates place CSBD at 2–7% in women and 3–10% in men.
That gap is real. But what happens at the clinical level is more revealing.
In specialized treatment clinics, only 5.3% of patients seeking CSBD treatment are women, despite women making up roughly a third of those actually affected (PMC, 2020). And this number has been recently receding further. Research published in PMC (2024) found that 68.2% of women with significant CSBD symptoms had never sought treatment for the condition. And across all genders, only 13.7% of high-risk individuals ever sought any treatment.
This is not because women experience less distress. It is because the shame of a woman having compulsive sexual behavior is layered differently.
The WHO's ICD-11 (2022) officially classifies CSBD as an impulse control disorder (not an addiction in the technical sense), characterized by a persistent pattern of failure to control intense, repetitive sexual impulses or urges, resulting in sexual behavior that causes marked distress or significant impairment lasting six months or more. The classification matters: CSBD is recognized, named, and treatable.
What It Actually Looks Like in Women
One reason women with CSBD do not recognize themselves in the clinical picture is that the clinical picture was drawn almost entirely from male patients.
Research comparing presentations by gender shows a clear divide. Men's compulsive sexual behavior tends toward pornography use (reported in 82% of male clinical cases) and solitary sexual activity. Women's patterns are different: 88% of female clinical cases involve compulsive interpersonal sexual activity: sex with other people, as the primary pattern.
Women are also more likely to experience what is sometimes called love addiction or romantic compulsivity, a pattern in which the compulsion centers not just on sex but on romantic connection, pursuit, and attachment. Research on love addiction shows research samples that are overwhelmingly female: in one study, 310 women and 19 men out of 329 total. The pattern is recognizable: an incessant need for a partner's presence, difficulty tolerating separation, a cycle of idealization followed by desperate pursuit when the connection feels threatened.
Women with CSBD are also significantly more likely to use sexual and romantic behavior as emotional regulation, to manage internal states that feel otherwise unmanageable. Research documents that 67% of individuals with CSBD report sadness or depression as a mood trigger for sexual acting out; 46% identify loneliness. For women, the sexual behavior is often less about desire and more about escape, numbing, or the temporary relief of feeling wanted.
This matters for recognition. A woman who uses romantic entanglement to manage depression does not think of herself as having a sexual behavior problem. She thinks of herself as someone who needs closeness, who falls hard, who cannot help herself.
Those descriptions are not wrong. But they are also, when the pattern persists, escalates, and resists her attempts to stop, pointing toward something that deserves a more specific name.
The Shame That Silences
Even when a woman suspects something is wrong, the shame of naming it is profound.
A 2024 study on the sexual double standard (N=705 women) found that 11% of women lie to their gynecologist about their sexual history, due to fear of judgment. A quarter of OBGYNs had expressed disapproval of patients' sexual practices. This judgemental approach of society towards female sexual behavior is seen as if it is under surveillance in ways that male sexual behavior simply is not.
When male sexual behavior is compulsive, the cultural framing tends toward weakness or disease. When female sexual behavior is compulsive, it is seen as a moral failure. A man with a sexual behavior problem may be pitied but accepted without any moral judgement. A woman with the same problem is judged.
This is not a perception. Research confirms that the prevailing double standard (male sexual activity normalized, female sexual activity pathologized) is one of the primary mechanisms preventing women from seeking help.
Brené Brown's Shame Resilience Theory, based on a qualitative study of 215 women, identifies shame (not guilt, not regret) as the primary emotional experience in this dynamic. Guilt says: I did something bad. Shame says: I am something bad. Brown notes: "The more we can separate 'I'm a good person, and I made a really bad choice,' the more we mitigate outcomes like addiction, depression, anxiety, and violence."
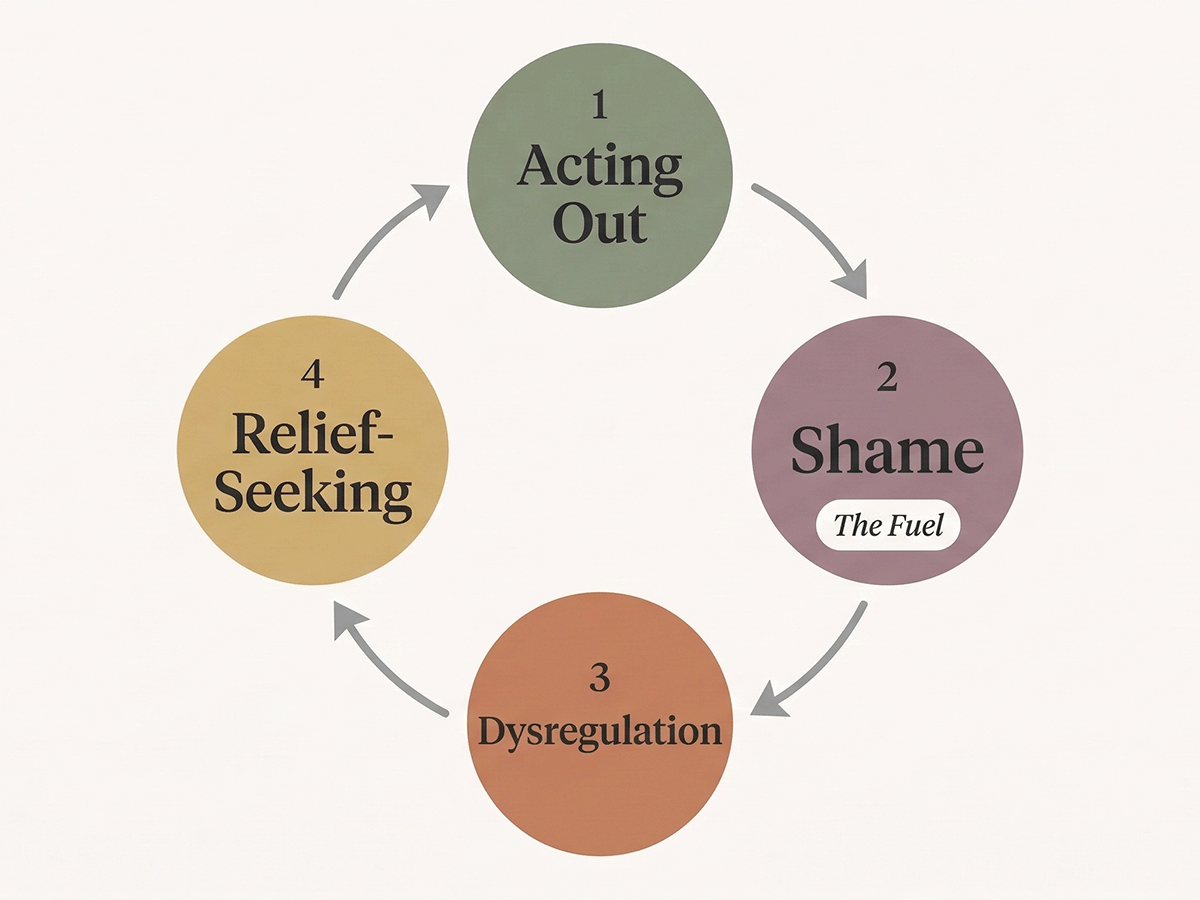
For women with CSBD, shame drives the cycle: the behavior triggers shame, the shame increases emotional dysregulation, and the dysregulation triggers further acting out. The shame is not just a consequence of the behavior. It becomes the fuel.
For South Asian Women, the Shame Is Layered Differently
For women from South Asian and Indian backgrounds (whether living in India or in diaspora communities in the UK, US, Sweden, or elsewhere), the shame of compulsive sexual behavior operates through specific cultural mechanisms.
Izzat (family honor) and sharam (shame) are interconnected constructs in South Asian culture that position family honor as maintained, in significant part, by female sexual conduct. Research from Howe & Sangar (2021) documents how South Asian women describe shame as "regulatory, sexist and oppressive and at the same time as helpful and protective", a complexity that captures just how deeply internalized these constructs become.
A 2024 PLOS Mental Health study on South Asian survivors in the UK found that South Asian women experience "an additional layer of shame" beyond that of other cultural groups. The fear is not just personal: it extends to family reputation, marriage prospects, the dowry system, and the possibility that information might reach family networks in the country of origin. One therapist in the study described it as: "The extra layer is the fear of reprisals, the fear of what will people think of you, the fear of ruining the family name."
For a South Asian woman reading this who is wondering whether her pattern constitutes a problem: the shame you feel about your sexual life may be cultural conditioning rather than evidence of compulsive behavior. Shame about entirely healthy sexuality is common in communities with strong sexual norms. CSBD requires something more specific: a loss of control, repeated failed attempts to stop, and functional impairment. The shame is not the diagnosis.
The Trauma Connection
For many women, compulsive sexual behavior is not a standalone pattern. It is connected to something older.
A 2025 study in Archives of Sexual Behavior found that PTSD symptoms moderate the relationship between childhood sexual abuse and compulsive sexual behavior, meaning that women with unresolved trauma or abuse can show compulsive behavior along with PTSD symptoms. Research comparing women and men with CSBD found that women showed higher rates of childhood maltreatment: sexual abuse (odds ratio: 2.9) and physical abuse (odds ratio: 3.7).
The compulsive behavior in trauma survivors often serves a function: regulating overwhelming traumatic emotions, re-enacting familiar attachment styles, or providing temporary escape from emotional pain that has no other exit. The behavior is not a moral failure. It is a coping strategy that once had a logic, and now has a cost.
Attachment patterns are also relevant. Research consistently links insecure attachment to CSBD, with anxious attachment showing the strongest connection. Adults with adverse childhood experiences who developed anxious attachment styles use sexual behavior to regulate the intense fear of abandonment that close relationships trigger. Studies on love addiction show a "strong significant correlation" with ambivalent attachment, the pattern of craving intimacy while dreading its loss.
And the mental health picture is complex: 90% of individuals seeking CSBD treatment have at least one comorbid psychiatric diagnosis. Depression, anxiety, PTSD, and eating disorders frequently co-occur, particularly in women.
What Actually Helps
CSBD in women responds to treatment, and the options keep growing.
Cognitive Behavioral Therapy (CBT) is the most researched approach for CSBD. Evidence shows significant reduction in compulsive sexual symptoms through psychoeducation, awareness of thoughts and emotional triggers, self-regulation training, and relapse prevention. For women whose CSBD is rooted in emotional regulation, CBT addresses the underlying thought patterns (the beliefs that "I need this to feel okay" or "I cannot tolerate this feeling without acting") and builds alternative coping strategies.
Trauma-Focused CBT (TF-CBT) and EMDR are particularly relevant when childhood trauma underlies the pattern. A 2024 randomized controlled trial on women survivors of childhood sexual abuse found both approaches significantly reduced trauma symptomatology: TF-CBT enhanced emotional regulation; EMDR significantly improved dissociation.
DBT (Dialectical Behavior Therapy) is a strong fit for women with CSBD given its emphasis on emotional regulation and distress tolerance, directly addressing the emotion dysregulation that research consistently identifies as central to women's compulsive sexual behavior.
Mindfulness-based interventions also show promise. A 2025 systematic review found that mindfulness programs significantly improved sexual distress and overall sexual wellbeing, and dispositional mindfulness was negatively associated with CSBD scores in women. Mindfulness brings the non-judgmental awareness that is the opposite of the shame-and-avoidance cycle.
Shame resilience work, drawing on Brené Brown's four-step framework of recognizing shame triggers, practicing critical awareness, reaching out, and speaking the shame, is not a standalone treatment but an essential bridge component. Shame is the primary barrier to recovery. Loosening shame's grip on identity, separating "I am this behavior" from "I do this behavior and I want to change", is where healing becomes possible.
Before You Diagnose Yourself
A note that matters, particularly for readers from cultural backgrounds with strong sexual norms:
Compulsive sexual behavior is not the same as a high libido or liberal sexual values. The distinction is not what you do or how often: it is whether you can choose to stop, whether the behavior aligns with your own values, whether you have tried and failed to control it, and whether it is causing significant distress or harm.
If you feel ashamed of your sexuality but can control your behavior and your sex life does not cause meaningful harm, the shame may be the problem, not the behavior. Cultural conditioning that teaches women their sexuality is inherently wrong creates a false diagnostic picture. Many South Asian women carry deep shame about desires and behaviors that are entirely healthy. That shame deserves attention. It is not evidence of CSBD.
If, on the other hand, you recognize a pattern of trying and failing to stop, of behavior that conflicts with your own values, of a cycle in which relief is always temporary and shame always follows. That recognition matters. You do not have to keep managing it alone.
You Are Not What You Have Done
I work in this field because I believe that every pattern has a history, and every history can be understood. The women I have worked with who struggle with compulsive sexual behavior are not broken. They are people who found a way to cope with pain, and who are ready, when they find the right support, to find better ways.
The shame of this experience does not have to be the ending of the conversation. It can be the beginning of one.
If any part of this article has named something you have been living with quietly, I want you to know: you are not alone, you are not beyond help, and the people who work in this area have heard it before. Speaking it (to a professional, in a support group, in whatever form feels survivable) is how the cycle begins to shift.
Shame grows in silence. It begins to lose its grip in light.
✦ Written with AI Assistance
The research and initial draft for this article were developed using Claude by Anthropic. Dr. Swapna Vithalkar reviewed and shaped the final content.


